


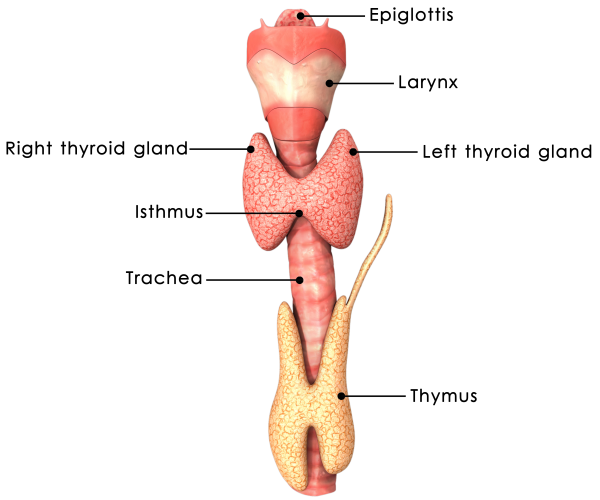
The thyroid gland is located on the front part of the neck below the thyroid cartilage (Adam's apple). The gland produces thyroid hormones, which regulate body metabolism. Thyroid hormones are important in regulating body energy, the body's use of other hormones and vitamins, and the growth and maturation of body tissues. Diseases of the thyroid gland can result in either production of too much (overactive thyroid disease or hyperthyroidism), or too little (underactive thyroid disease or hypothyroidism) thyroid hormone, thyroid nodules, and/or goiter. All types of thyroid problems are much more common in women than in men.
Production of thyroid hormones: The process of hormone synthesis begins in a part of the brain called the hypothalamus. The hypothalamus releases thyrotropin-releasing hormone (TRH). The TRH travels through the venous plexus located in the pituitary stalk to the pituitary gland, also in the brain. In response, the pituitary gland then releases thyroid-stimulating hormone (TSH) into the blood. The TSH travels to the thyroid gland and stimulates the thyroid to produce the two thyroid hormones, L-thyroxine (T4) and triiodothyronine (T3). The thyroid gland also needs adequate amounts of dietary iodine to be able to produce T4 and T3.
Regulation of thyroid hormone production: To prevent the overproduction or underproduction of thyroid hormones, the pituitary gland can sense how much hormone is in the blood and adjust the production of hormones accordingly. For example, when there is too much thyroid hormone in the blood, TRH and TSH production are both decreased. The sum effect of this is to decrease the amount of TSH released from the pituitary gland and to reduce production of thyroid hormones from the thyroid gland to restore the amount of thyroid hormone in the blood to normal. Defects in these regulatory pathways may result in hypothyroidism (underactive thyroid problem) or hyperthyroidism (overactive thyroid problem).
Thyroid goiter: Thyroid goiter is any enlargement of the thyroid that can occur with hyperthyroidism or hypothyroidism but also with benign and malignant (cancerous) nodules. Worldwide, the most common cause of goiter is iodine deficiency. Although it used to be very common in the U.S., it is now less common with the use of iodized salt. Multiple nodules in the thyroid are very common, but only about 5% of the nodules are a thyroid cancer. Thyroid cancer is diagnosed after a thyroid ultrasound exam and a needle aspiration biopsy of the nodule.
HYPOTHYROIDISM IN PREGNANCY
Newly diagnosed hypothyroidism in pregnancy is rare because most women with untreated hypothyroidism do not ovulate or produce mature eggs in a regular manner, which makes it difficult for them to conceive.
It is a difficult new diagnosis to make based on clinical observation. The signs and symptoms of hypothyroidism (fatigue, poor attention span, weight gain, numbness, and tingling of the hands or feet) are also prominent symptoms of a normal pregnancy. Undiagnosed hypothyroidism during pregnancy increases the chance of stillbirth or growth retardation of the fetus. It also increases the chance that the mother may experience complications of pregnancy such as anemia, eclampsia, and placental abruption.
Probably the largest group of women who will have hypothyroidism during pregnancy are those who are currently on thyroid hormone replacement. The ideal thyroxine replacement dose (for example, levothyroxine [Synthroid, Levoxyl, Levothroid, Unithroid]) may rise by 25% to 50% during pregnancy. It is important to have regular checks of T4 and TSH blood levels as soon as pregnancy is confirmed; and frequently through the first 20 weeks of pregnancy to make sure the woman is taking the correct medication dose.
HYPERTHYROIDISM IN PREGNANCY
Newly diagnosed hyperthyroidism occurs in about 1 in 2,000 pregnancies. Grave's disease accounts for 95% of cases of hyperthyroidism newly diagnosed during pregnancy.
As with hypothyroidism, many symptoms of mild hyperthyroidism mimic those of normal pregnancy. However, anyone experiencing symptoms such as significant weight loss, vomiting, increased blood pressure, or persistently fast heart rate should have blood tests to evaluate whether hyperthyroidism is present.
Untreated hyperthyroidism does cause fetal and maternal complications including poor weight gain and tachycardia (an abnormally fast heart rate). Treatment of hyperthyroidism during pregnancy is primarily medical. Propylthiouracil or methimazole (Tapazole) are the usual first-line agents to block the synthesis of thyroid hormone. They appear to be equally effective and have the same rate of side effects, which are not increased in pregnancy. Iodine will cross the placenta, so its use in either a thyroid scan or in treatment with radioactive iodine is prohibited in pregnancy.
One positive note for women with hyperthyroidism is that those with Grave's disease or Hashimoto's thyroiditis may have improvement in their symptoms during pregnancy.
GOITER IN PREGNANCY
It is common for a goiter to enlarge slightly during pregnancy. It is more common when the mother lives in an area of iodine deficiency. In the United States, the average intake of iodine is adequate but can be low if someone avoids consumption of milk, eggs, and iodized salt. Not all prenatal vitamins contain iodine, but it is recommended that only prenatal vitamins that contain iodine should be used during pregnancy.
POSTPARTUM THYROID DISEASE
Some women may have thyroiditis that usually occurs within 3 to 6 months after giving birth. It also may occur after a miscarriage. The classic clinical picture is a woman who will first have symptoms of hyperthyroidism, followed by hypothyroidism, culminating in normal thyroid function.
Women with type I diabetes have a 25% risk of developing postpartum thyroid dysfunction.
Consult your doctor if you have symptoms of hypothyroidism or hyperthyroidism after pregnancy or miscarriage.
